What is an ulcer?
An ulcer is damage to the inner lining (the mucosa) of the stomach or the upper part of the intestine (duodenum). A bacterium, Helicobacter pylori, is the main cause of ulcers in this area.
Why do people get ulcers?
The most common cause is infection with Helicobacter pylori bacteria and this is responsible for up to 90 per cent of all cases of peptic ulceration.
The second most common cause is damage inflicted by aspirin (eg Disprin) or non-steroidal anti-inflammatory drugs (NSAIDs, such as diclofenac (eg Voltarol) or naproxen (eg Synflex)) used by many for arthritis, rheumatism, backache, headaches and period pain.
Ulcers can also occur in people weakened by severe disease (such as chronic respiratory disease or major trauma). This is thought to result from poor oxygenation to the lining of the stomach.
Occasionally (in Europeans), a stomach ulcer is caused by cancer and rarely, some other specific illness is found to be responsible. Such conditions include:
- Excessive production of hydrochloric acid in the stomach (Zollinger-Ellison syndrome)
- Crohn’s disease (an inflammatory condition affecting any part of the gut).
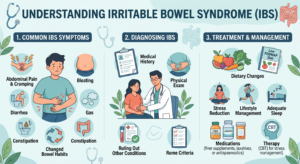
What does an ulcer feel like?
This varies greatly from person to person. Many people never realise that they have an ulcer. Others feel pain or a burning sensation in their upper abdomen. The symptoms are often described as indigestion, heartburn, hunger pangs or dyspepsia.
Some sufferers find that eating actually helps settle their discomfort for a while, others find it makes them worse. Citrus drinks, spicy and smoked foods can make the pain worse.Finally, it is important to stress that most people with a stomach ache do not have ulcers.An ulcer is potentially dangerous – the warning signs are:
- difficulty swallowing or regurgitation
- persistent nausea and vomiting
- vomiting blood or vomit with the appearance of coffee grounds
- black or tar-like stools
- unintended weight loss
- anaemia (paleness and fatigue)
- sudden, severe and incapacitating abdominal pains.
What can I do to help myself?
Smoking and drinking alcohol puts you at greater risk of developing an ulcer. It’s a good idea to stop smoking and moderate your alcohol intake. If for any reason you have an increased risk of ulcers, it is important to seek advice before considering NSAIDs or aspirin.
If you experience the symptoms of an ulcer, consult our doctor. You may need a thorough examination in hospital with a gastroscopy. This is a safe and commonly performed procedure that will help our doctor decide whether your symptoms are due to an ulcer or something else.
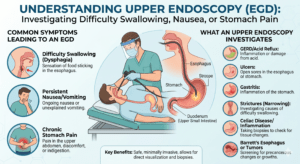
How do our doctor’s make a diagnosis?
The diagnosis can only be definitely confirmed or excluded by a gastroscopy. A gastroscopy (or upper GI endoscopy) involves the visualisation of the lining of your gullet (oesophagus), stomach and duodenum with a small fibre-optic camera that can be swallowed.
The gastroscopy is more helpful in diagnosis if it is performed before you take any acid-reducing medication.
An X-ray examination (involving a Barium meal) can also be used, but it is not quite as reliable or helpful a diagnostic tool as a gastroscopy. It does not offer any opportunity to take tissue samples (biopsies) for microscopic diagnosis of tissue abnormalities and infection.
What is Helicobacter pylori?
Helicobacter pylori is a minute bacteria living inside and under the lining of the stomach. The groups most often affected are:
- elderly people
- people in developing countries.
Those who carry this bacteria today have most probably been infected during childhood. The risk of acquiring infection for an adult is modest – less than 1 per cent every year.
Helicobacter pylori in itself does not usually cause any ulcer symptoms. Nevertheless, this bacteria is the most common cause of ulcers in the stomach and the duodenum.
The bacteria may also have a role in the development of cancer of the stomach. Helicobacter pylori infection can be eliminated by taking antibiotics. There is about an 80 per cent chance of successful treatment of the infection and a cure for the ulcer.If the bacteria is not eliminated, most people get a recurrence of their ulcer after a short period of time.
How to detect an infection by Helicobacter pylori?
Gastroscopy, followed by biopsy of the lining of the stomach (the mucosa) can allow the bacteria, inflammation, and tissue abnormalities to be assessed under a microscope. From a biopsy, tissue from the mucosa can be cultured and an indicator fluid (a urease test) can verify the presence of bacteria. ‘Breath test’ examination: the expired air is tested, after ingestion of a small amount of labelled urea (in crystalline form).
Blood sample: if you have, or have had, Helicobacter pylori, it can be detected by the presence of antibodies in your blood.
Stool sample: this technique is not yet perfected. But the method involves tracing bacterial DNA in stool samples.
Who should be screened and treated for Helicobacter pylori?
These questions continue to be debated.
- All patients with a proven ulcer of the stomach or duodenum should be tested, and treated if the bacteria is found.
- People under the age of 45 with ulcer-like symptoms can avoid gastroscopy by choosing the breath test. If it is positive for Helicobacter pylori infection the patient should be treated with antibiotics.
- People with diagnosed lymphatic cancer of the stomach (very rare) should be examined and, if the bacteria are present, treated.
- People with diagnosed early stages of cancer of the stomach should be examined and treated if the bacteria are present.
Almost everyone with a past history of proven ulcers in the duodenum has Helicobacter pylori and, therefore, it has been proposed that these people could be treated without testing. Anyone with ulcer-like symptoms, but a normal gastroscopy, will not benefit from testing or treatment.
Which types of medicine can cause ulcers and ulcer complications?
Aspirin (eg Disprin) and non-steroidal anti-inflammatory drugs (NSAIDs such as diclofenac or naproxen) can cause ulcers, but only a small proportion of the people taking these drugs develop an ulcer.
Some people have a very high sensitivity to aspirin and NSAIDs and such people should not take this sort of medication. If you have previously had a bleeding ulcer, you must not take medicine that includes aspirin (acetylsalicylic acid) or NSAIDs.
Who is at risk from treatment with aspirin (acetylsalicylic acid) and NSAIDs?
- People older than 60 – the risk increases with age.
- If you have had a previous ulcer, the risk is high.
If you are taking anticoagulants (blood-thinning treatment) at the same time, bleeding is more likely and more serious when it occurs. Oral corticosteriods (such as prednisolone (eg Precortisyl)) increase the chances of gastric irritation and ulcers.
The larger the dose of aspirin or NSAIDs the greater the risk. The longer duration of the treatment, the greater the risk.
Can I reduce the risk from aspirin or NSAIDs?
If you are predisposed to this problem, the risk is not diminished by taking the medication:
- on a full stomach
- as a dissolved or glazed tablet (‘enteric coated’)
- through other routes, such as suppositories or injections.
However, acid-reducing medication (H2 inhibitors, such as ranitidine (eg Zantac) or nizatidine (Axid)) does diminish the ulcer risk associated with aspirin and NSAIDs.
Treatment with another medicine called misoprostol (eg Cytotec) offers protection for the mucosa and is also potentially beneficial. Misoprostol can cause diarrhoea but this tendency varies from person to person.
Can you avoid treatment with NSAIDs?
Pain can often be alleviated by medication that does not predispose to peptic ulceration. Paracetamol (eg Panadol) may be worth trying in this respect, as it is not associated with peptic ulceration. Headaches, migraine and chronic abdominal pain are conditions for which NSAIDs can easily be substituted by other painkillers.
In the case of gout, acute attacks can be treated with other drugs such as colchicine instead of NSAIDs.
For arthritis, traditional NSAIDs can be replaced with a new sub-group of NSAIDS called cox-2 selective inhibitors, eg celecoxib (Celebrex) or etoricoxib (Arcoxia). These have a lower risk of serious gastrointestinal side effects and can be used for people at high risk, eg people over 65 years of age or those taking other medicines that increase the risk of ulcers. However, as these medicines can still cause ulcers, they should not be used in people with an active ulcer, and only after careful consideration in people with a history of ulcers.
Can you avoid treatment with aspirin?
In many cases, aspirin can be substituted with other medication, such as paracetamol, which will not predispose to peptic ulcers and yet offer the same therapeutic effect. In the case of aspirin, paracetamol is equally effective with no ulcer risk. When low dose aspirin (eg Caprin 75mg) is prescribed for the reduction of cardiovascular risk (complications arising from ‘hardening of the arteries’ – atherosclerosis), a balance needs to be struck between the risk of heart/arterial disease and the risk of peptic ulceration.
If you have a history of peptic ulcers, your cardiovascular risk can be reduced with alternatives to aspirin, such as dipyridamole (Persantin) or Clopidogrel (Plavix).
The relative risk of each of these conditions and their management varies from person to person, so it is always worth talking it over with our doctor.