There's a category of symptoms that's easy to rationalize away — a little trouble swallowing solid food, nausea that shows up without a clear reason, or a persistent dull ache in the upper abdomen. You figure it's stress. Or something you ate. Or just "getting older."
But when these symptoms keep coming back — or when they've quietly become the new normal over months — they deserve a direct answer. Not more antacids. Not another round of "wait and see." A direct look. That's exactly what an upper endoscopy in Houston provides.

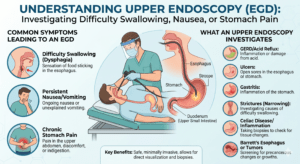
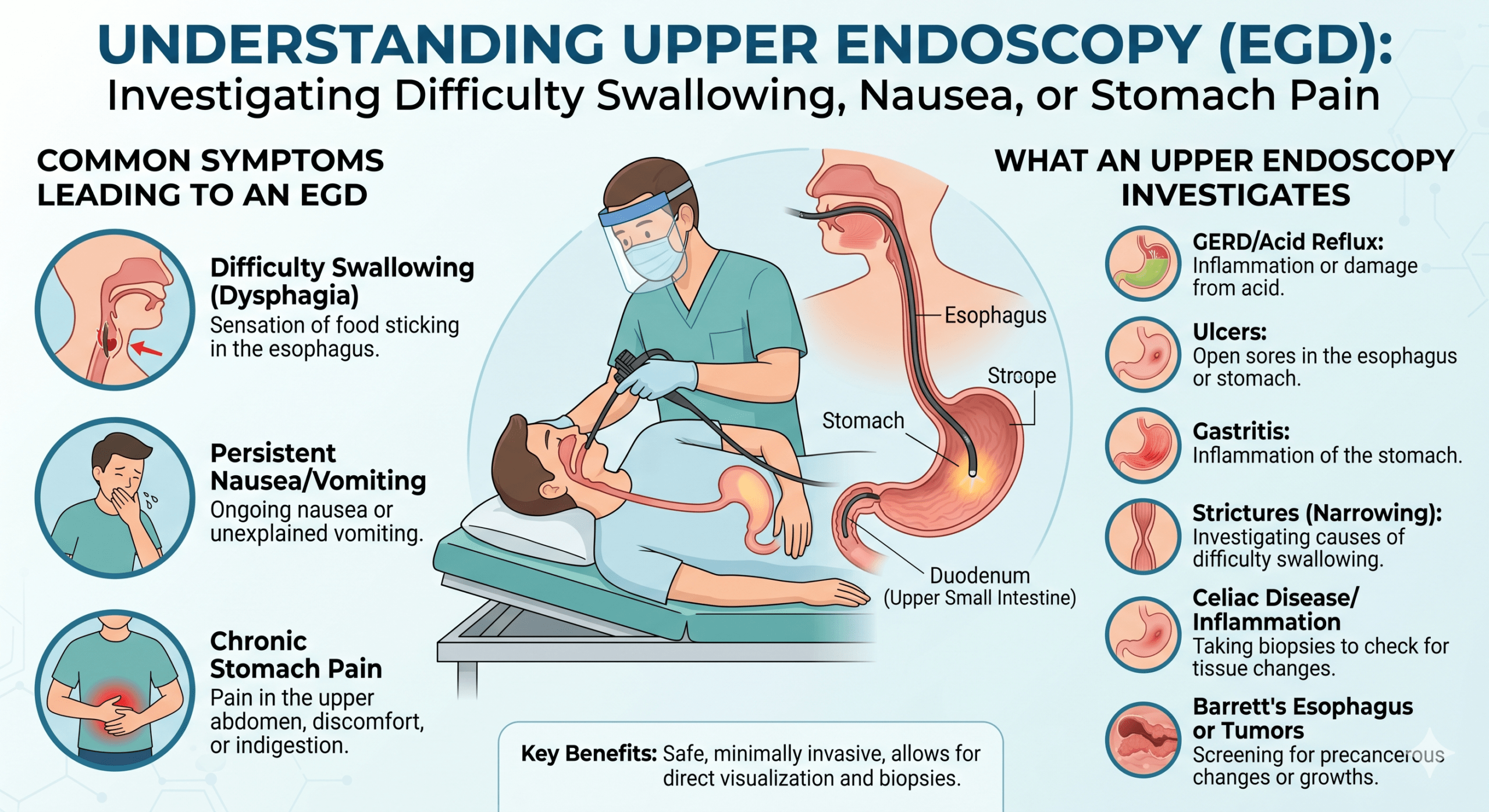
Difficulty Swallowing: Never Normalize It
Dysphagia — difficulty swallowing — is one of the GI symptoms that most warrants prompt attention. The sensation can range from mild (food feels like it's moving slowly or sticking briefly in the throat or chest) to significant (avoiding certain textures entirely, or food genuinely getting stuck). It's progressive in many cases — and that progression matters, because the conditions causing it don't typically improve on their own.
Narrowing of the esophagus — one of the most common causes of progressive swallowing difficulty. They can result from chronic acid damage from GERD, radiation, or surgical scarring. Upper endoscopy diagnoses them and can treat them during the same procedure through esophageal dilation, where the narrowed area is carefully stretched.
Structural abnormalities that partially obstruct the esophagus. A Schatzki's ring — a thin band of tissue where the esophagus meets the stomach — is a common cause of intermittent food impaction in adults, and like strictures, can often be treated endoscopically.
An increasingly recognized condition where immune cells accumulate in the esophageal lining, making it stiff, ringed, or furrowed. It often appears in adults with a personal or family history of allergic conditions. Diagnosis requires upper endoscopy with biopsies — and EoE responds well to specific treatment once identified.
A motility disorder in which the lower esophageal sphincter fails to relax during swallowing, causing food to accumulate in the esophagus. Upper endoscopy is part of the diagnostic workup alongside other tests.
Esophageal cancer, while less common, can present with progressive difficulty swallowing solid foods, often with weight loss. Early detection vastly improves outcomes. Anyone with progressive dysphagia — particularly with weight loss — should be evaluated without delay.
Persistent Nausea: When It's More Than Temporary
Nausea that lasts for weeks without a clear cause — not tied to a specific illness, travel, or medication — is worth investigating. Chronic nausea can originate from multiple GI structures that upper endoscopy directly evaluates.
Delayed stomach emptying produces persistent nausea, early satiety (feeling full very quickly), bloating, and sometimes vomiting. While a gastric emptying study is the standard test, upper endoscopy is often done first to rule out structural causes.
Ulcers in the stomach or duodenum frequently present with nausea alongside epigastric pain — they're directly visible during EGD and can be biopsied for H. pylori testing. Gastritis (inflammation of the stomach lining) may cause nausea with or without pain and is accurately diagnosed through endoscopy with biopsy.
Found in a significant portion of adults, it can cause chronic nausea and upper abdominal discomfort, contributes directly to ulcer formation, and — in long-term untreated cases — raises gastric cancer risk.
Upper Abdominal Pain That Won't Quit
That burning, gnawing, or pressure sensation in the middle of the upper abdomen — sometimes called epigastric pain — is one of the most common symptoms that leads Houston patients to upper endoscopy.
A frequent cause. Ulcers often produce pain relieved by eating (especially duodenal ulcers) or worsened by it (gastric ulcers). Regular NSAID use — ibuprofen, naproxen — is a leading cause, as is H. pylori.
GERD may cause upper abdominal burning that patients describe as stomach pain rather than heartburn. Functional dyspepsia — discomfort without a structural or inflammatory cause — is diagnosed after other conditions are excluded, and upper endoscopy is typically part of that exclusion in adults over 45.
These can produce upper abdominal pain requiring further evaluation with endoscopic ultrasound or other tools if the initial upper endoscopy is unremarkable.
Why Imaging Alone Isn't Enough

A common question: "Can't a CT scan or ultrasound tell you what's going on?" Imaging studies are valuable but have significant blind spots for the upper GI tract.
CT scans see large structural changes but miss early mucosal disease — the changes in the esophagus, stomach, and duodenal lining that are the most common cause of symptoms and the most treatable when caught early. An ultrasound sees the gallbladder and liver, but not the esophagus or stomach lining.
Upper endoscopy provides direct visualization of the mucosal surface — where ulcers, Barrett's esophagus, H. pylori-related gastritis, and early cancers live.
"There's no substitute for looking at the tissue directly. Upper endoscopy lets your Houston gastroenterologist see the mucosal layer in real time — and take biopsies or treat a problem during the very same procedure."
What to Expect If Your Doctor Recommends Upper Endoscopy

- Before — fasting, no bowel prep You'll fast for at least eight hours beforehand — nothing to eat or drink, except small sips of water for essential medications. Unlike a colonoscopy, no bowel prep is required.
- During — sedation and a short procedure You'll receive sedation through an IV, and the procedure itself takes just 10 to 20 minutes. You won't feel it.
- After — recovery and results You wake up in recovery, spend about an hour there, and go home with someone driving you. Most people feel fully normal by the next day, aside from possible mild throat soreness or bloating. If biopsies were taken, results return within three to seven business days and your GI team follows up directly.
Before you leave, your Houston gastroenterologist will tell you what was found. Have questions first? Visit our FAQ page or read more on our blog.
Getting Evaluated at Your GI Center in Houston
Your GI Center serves patients throughout the Brazosport area — Lake Jackson, Clute, Freeport, Angleton, Brazoria — as well as Pearland, Friendswood, League City, and the South Houston corridor. Our Lake Jackson and Houston endoscopy centers perform upper endoscopies with the same experienced team, advanced equipment, and patient-centered approach at both locations.
"Don't keep rationalizing persistent symptoms. Difficulty swallowing, chronic nausea, and stubborn upper abdominal pain all have answers — and an upper endoscopy is often the most direct way to find them."
Get a Clear Answer With Upper Endoscopy in Houston
Our board-certified Houston gastroenterologists, Dr. Nizam Meah and Dr. U. Siddiqui, perform upper endoscopy at on-site endoscopy centers in South Houston and near Lake Jackson. Persistent swallowing trouble, nausea, or upper stomach pain deserves a direct look. Appointment requests are typically returned within three hours during business hours.