You've had unpredictable bowel habits for months. Some days it's diarrhea, some days it's constipation that won't let up, and some days it's both — sometimes in the same week. Your abdomen cramps, you feel bloated, and there are foods you've quietly started avoiding because you never know how your body will react.
You've Googled it. IBS keeps coming up. But you're not sure, and you'd rather know for certain than assume. Here's what your Houston gastroenterologist wants you to understand about irritable bowel syndrome — what it is, what it isn't, and why getting properly evaluated matters even when you think you already have the answer.

What IBS Actually Is
Irritable bowel syndrome is a functional gastrointestinal disorder. That means there's no structural damage, no inflammation, and no identifiable disease process in the bowel — but the bowel isn't functioning normally. Signals between the gut and the brain are disrupted, causing the colon to respond abnormally to food, stress, hormonal changes, and other triggers.
IBS is classified into subtypes based on the dominant bowel pattern:
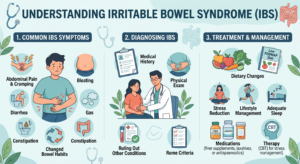
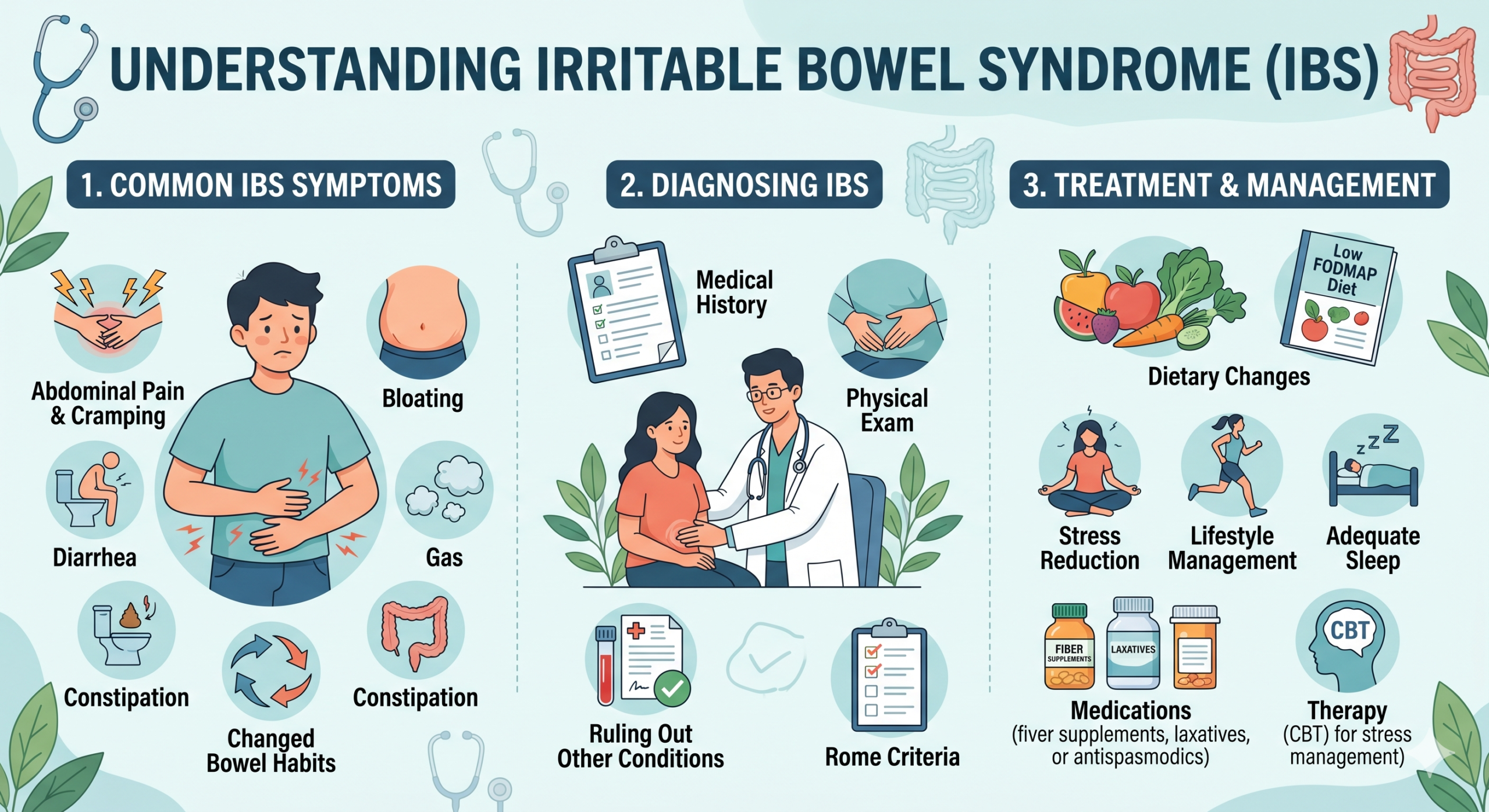
The hallmark symptom is abdominal pain or cramping related to bowel function — triggered by eating, relieved (at least temporarily) by a bowel movement, or tied to a change in stool frequency or consistency. Bloating and abdominal distension are very common companions.
What IBS Is Not
This distinction matters enormously: IBS is not the same as inflammatory bowel disease (IBD). IBD — which includes Crohn's disease and ulcerative colitis — involves genuine, chronic inflammation of the intestinal wall, carries a risk of complications such as strictures and fistulas, and requires a different category of treatment entirely.
Many patients come to our Houston practice having self-diagnosed with IBS when they actually have IBD — or having been told they have IBS when something else is going on. The symptoms can overlap enough to create real confusion. That's precisely why a proper evaluation matters.
IBS does not cause rectal bleeding, significant weight loss, symptoms that wake you from sleep, or fevers. When any of these are present, the diagnosis is almost certainly not simple IBS and warrants a more thorough investigation.
Who Gets IBS — and Why Houston Adults Over 45 Aren't Immune
IBS affects roughly 10 to 15 percent of adults. It's more common in women and often begins in early adulthood — but it can develop or change in character at any age. Adults in their 40s and 50s who notice a change in their bowel patterns sometimes assume it's "just getting older." Sometimes it is. Sometimes it's IBS. And sometimes it's something that needs to be ruled out before landing on that conclusion.
Post-infectious IBS — a subset that develops after a significant GI illness such as food poisoning — is increasingly recognized and can begin in adulthood. The COVID-19 pandemic left a meaningful number of people with altered GI motility and function that shares features with IBS.
How IBS Is Diagnosed

There's no definitive test for IBS. The diagnosis is made clinically — based on the pattern of symptoms — using the Rome IV criteria, which require recurrent abdominal pain on average at least one day per week over the past three months.
That pain must be associated with at least two of the following: related to defecation, associated with a change in stool frequency, or associated with a change in stool form.
But before a Houston gastroenterologist diagnoses IBS, other conditions need to be excluded.
Depending on your symptom profile, age, and history, the workup to exclude other causes may involve:
- Blood work — to evaluate for inflammation, celiac disease, thyroid function, and other conditions.
- Stool studies — to look for infection or inflammation.
- Colonoscopy in Houston — particularly for adults over 45 or those with symptoms that could indicate IBD or colorectal pathology.
"In adults over 45, IBS is a diagnosis of exclusion. That means you're not relying on your own — or anyone else's — assumption that it's IBS until other explanations have been appropriately ruled out."
The Role of Colonoscopy in IBS Evaluation
For patients 45 and older with new or changed bowel symptoms, colonoscopy is often part of the evaluation — not because IBS is visible on colonoscopy (it isn't), but because it's the most direct way to rule out inflammatory bowel disease, microscopic colitis, colorectal cancer, and other structural causes that produce similar symptoms.
Microscopic colitis — where inflammation is visible only under the microscope, not to the naked eye — is a common cause of chronic, watery diarrhea in adults over 40 and is frequently mistaken for IBS until biopsies taken during colonoscopy reveal it. It responds very well to specific treatment — but only once it's correctly diagnosed.
Treatment Options for IBS
IBS management focuses on reducing the frequency and severity of symptoms. There's no cure, but most patients achieve meaningful control with the right combination of dietary, lifestyle, and medical interventions.

- Diet — often the most impactful lever The low-FODMAP diet temporarily restricts certain fermentable carbohydrates the gut poorly absorbs. It has the most robust evidence base for IBS and reduces symptoms in roughly 50 to 70 percent of patients who follow it properly. It's best done with guidance from a registered dietitian.
- The gut-brain connection The gut has its own extensive nervous system and communicates bidirectionally with the brain. Stress, anxiety, and depression all influence gut motility and sensitivity. Cognitive behavioral therapy, gut-directed hypnotherapy, and mindfulness have evidence supporting their use in IBS — alongside or instead of medication.
- Medications matched to your subtype Depending on your IBS subtype, options range from antispasmodics and fiber supplements to prescription agents targeting specific gut receptors. Low-dose antidepressants are sometimes used for their effects on gut-brain signaling rather than mood.
Your Houston gastroenterologist will work with you to build a plan tailored to your specific symptom pattern and history — not a one-size-fits-all protocol. Have questions first? Visit our FAQ page or read more on our blog.
Getting Evaluated for IBS in Houston at Your GI Center
Your GI Center serves patients from South Houston, Pearland, Friendswood, Missouri City, and the Brazosport area including Lake Jackson, Clute, and Angleton. Our Houston gastroenterologists evaluate IBS regularly and have the diagnostic tools to distinguish it from the conditions that need to be excluded first.
"If you've been managing gut symptoms for months without a formal evaluation, this is the point where guessing stops being reasonable. An evaluation gives you answers — and a clear treatment path — that self-diagnosis doesn't."
Get a Clear IBS Diagnosis in Houston at Your GI Center
Our board-certified Houston gastroenterologists, Dr. Nizam Meah and Dr. U. Siddiqui, evaluate IBS and the conditions that mimic it across the Houston area and Brazosport region. We'll give you a clear diagnosis and a treatment plan based on what's actually going on. Appointment requests are typically returned within three hours during business hours.