What is the Esophagus?
The esophagus is a hollow tube that carries food and liquids from the throat to the stomach. When a person swallows, the muscular walls of the esophagus contract to push food down into the stomach. Glands in the lining of the esophagus produce mucus, which keeps the passageway moist and makes swallowing easier. The esophagus is located just behind the trachea (windpipe). In an adult, the esophagus is about 10 inches long.
What is Cancer?
Cancer is a disease that affects cells, the body’s basic unit of life. To understand any type of cancer, it is helpful to know about normal cells and what happens when they become cancerous.
The body is made up of many types of cells. Normally, cells grow, divide, and produce more cells when they are needed. This process keeps the body healthy and functioning properly. Sometimes, however, cells keep dividing when new cells are not needed. The mass of extra cells forms a growth or tumor. Tumors can be benign or malignant.
Benign tumors are not cancer. They usually can be removed and, in most cases, they do not come back. Cells in benign tumors do not spread to other parts of the body. Most important, benign tumors are rarely a threat to life. Malignant tumors are cancer. Cells in malignant tumors are abnormal and divide without control or order. These cancer cells can invade and destroy the tissue around them. Cancer cells can also break away from a malignant tumor and enter the bloodstream or lymphatic system (the tissues and organs that produce, store, and carry white blood cells that fight infection and other diseases). This process, called metastasis, is how cancer spreads from the original (primary) tumor to form new (secondary) tumors in other parts of the body.
Cancer that begins in the esophagus (also called esophageal cancer) is divided into two major types, squamous cell carcinoma and adenocarcinoma, depending on the type of cells that are malignant. Squamous cell carcinomas arise in squamous cells that line the esophagus. These cancers usually occur in the upper and middle part of the esophagus. Adenocarcinomas usually develop in the glandular tissue in the lower part of the esophagus. The treatment is similar for both types of esophageal cancer.
If the cancer spreads outside the esophagus, it often goes to the lymph nodes first. (Lymph nodes are small, bean-shaped structures that are part of the body’s immune system.) Esophageal cancer can also spread to almost any other part of the body, including the liver, lungs, brain, and bones.
Risk Factors
The exact causes of cancer of the esophagus are not known. However, studies show that any of the following factors can increase the risk of developing esophageal cancer:
- Age. Esophageal cancer is more likely to occur as people get older; most people who develop esophageal cancer are over age 60.
- Sex. Cancer of the esophagus is more common in men than in women.
- Tobacco Use.Smoking cigarettes or using smokeless tobacco is one of the major risk factors for esophageal cancer.
- Alcohol Use. Chronic and/or heavy use of alcohol is another major risk factor for esophageal cancer. People who use both alcohol and tobacco have an especially high risk of esophageal cancer. Scientists believe that these substances increase each other’s harmful effects.
- Barrett’s Esophagus. Long-term irritation can increase the risk of esophageal cancer. Tissues at the bottom of the esophagus can become irritated if stomach acid frequently “backs up” into the esophagus — a problem called gastric reflux. Over time, cells in the irritated part of the esophagus may change and begin to resemble the cells that line the stomach. This condition, known as Barrett esophagus, is a premalignant condition that may develop into adenocarcinoma of the esophagus.
- Other Types of Irritation. Other causes of significant irritation or damage to the lining of the esophagus, such as swallowing lye or other caustic substances, can increase the risk of developing esophageal cancer.
- Medical History. Patients who have had other head and neck cancers have an increased chance of developing a second cancer in the head and neck area, including esophageal cancer.
Having any of these risk factors increases the likelihood that a person will develop esophageal cancer. Still, most people with one or even several of these factors do not get the disease. And most people who do get esophageal cancer have none of the known risk factors.
Identifying factors that increase a person’s chances of developing esophageal cancer is the first step toward preventing the disease. We already know that the best ways to prevent this type of cancer are to quit (or never start) smoking cigarettes or using smokeless tobacco and to drink alcohol only in moderation. Researchers continue to study the causes of esophageal cancer and to search for other ways to prevent it. For example, they are exploring the possibility that increasing one’s intake of fruits and vegetables, especially raw ones, may reduce the risk of this disease.
Researchers are also studying ways to reduce the risk of esophageal cancer for people with Barrett’s esophagus.
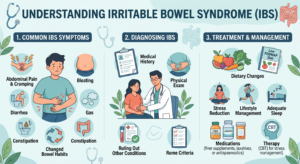
Recognizing Symptoms
Early esophageal cancer usually does not cause symptoms. However, as the cancer grows, symptoms may include:
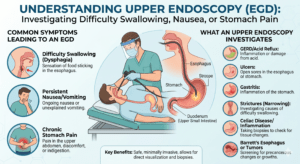
- Difficult or painful swallowing
- Severe weight loss
- Pain in the throat or back, behind the breastbone or between the shoulder blades
- Hoarseness or chronic cough
- Vomiting
- Coughing up blood
These symptoms may be caused by esophageal cancer or by other conditions. It is important to check with our doctor.
Diagnosing Esophageal Cancer
To help find the cause of symptoms, our doctor evaluates a person’s medical history and performs a physical exam. The doctor usually orders a chest x-ray and other diagnostic tests. These tests may include the following:
- A barium swallow (also called an esophagram) is a series of x-rays of the esophagus. The patient drinks a liquid containing barium, which coats the inside of the esophagus. The barium makes any changes in the shape of the esophagus show up on the x-rays.
- Esophagoscopy (also called endoscopy) is an examination of the inside of the esophagus using a thin lighted tube called an endoscope. An anesthetic (substance that causes loss of feeling or awareness) is usually used during this procedure. If an abnormal area is found, the doctor can collect cells and tissue through the endoscope for examination under a microscope. This is called a biopsy. A biopsy can show cancer, tissue changes that may lead to cancer, or other conditions.
Staging The Disease
If the diagnosis is esophageal cancer, our doctor needs to learn the stage (or extent) of disease. Staging is a careful attempt to find out whether the cancer has spread and, if so, to what parts of the body. Knowing the stage of the disease helps our doctor plan treatment. Listed below are descriptions of the four stages of esophageal cancer.
- Stage I. The cancer is found only in the top layers of cells lining the esophagus.
- Stage II. The cancer involves deeper layers of the lining of the esophagus, or it has spread to nearby lymph nodes. The cancer has not spread to other parts of the body.
- Stage III. The cancer has invaded more deeply into the wall of the esophagus or has spread to tissues or lymph nodes near the esophagus. It has not spread to other parts of the body.
- Stage IV. The cancer has spread to other parts of the body. Esophageal cancer can spread almost anywhere in the body, including the liver, lungs, brain, and bones.
Some tests used to determine whether the cancer has spread include:
- CAT (or CT) scan (computed tomography). A computer linked to an x-ray machine creates a series of detailed pictures of areas inside the body.
- Bone scan. This technique, which creates images of bones on a computer screen or on film, can show whether cancer has spread to the bones. A small amount of radioactive substance is injected into a vein; it travels through the bloodstream, and collects in the bones, especially in areas of abnormal bone growth. An instrument called a scanner measures the radioactivity levels in these areas.
- Bronchoscopy. The doctor puts a bronchoscope (a thin, lighted tube) into the mouth or nose and down through the windpipe to look into the breathing passages.
Treatment
Treatment for esophageal cancer depends on a number of factors, including the size, location, and extent of the tumor, and the general health of the patient. Patients are often treated by a team of specialists, which may include a gastroenterologist (a doctor who specializes in diagnosing and treating disorders of the digestive system), surgeon (a doctor who specializes in removing or repairing parts of the body), medical oncologist (a doctor who specializes in treating cancer), and radiation oncologist (a doctor who specializes in using radiation to treat cancer). Because cancer treatment may make the mouth sensitive and at risk for infection, our doctors often advise patients with esophageal cancer to see a dentist for a dental exam and treatment before cancer treatment begins.
Many different treatments and combinations of treatments may be used to control the cancer and/or to improve the patient’s quality of life by reducing symptoms.
- Surgery is the most common treatment for esophageal cancer. Usually, the surgeon removes the tumor along with all or a portion of the esophagus, nearby lymph nodes, and other tissue in the area. (An operation to remove the esophagus is called an esophagectomy.) The surgeon connects the remaining healthy part of the esophagus to the stomach so the patient is still able to swallow. Sometimes, a plastic tube or part of the intestine is used to make the connection. The surgeon may also widen the opening between the stomach and the small intestine to allow stomach contents to pass more easily into the small intestine. Sometimes surgery is done after other treatment is finished.
- Radiation therapy, also called radiotherapy, involves the use of high-energy rays to kill cancer cells. Radiation therapy affects cancer cells in the treated area only. The radiation may come from a machine outside the body (external radiation) or from radioactive materials placed in or near the tumor (internal radiation). A plastic tube may be inserted into the esophagus to keep it open during radiation therapy. This procedure is called intraluminal intubation and dilation. Radiation therapy may be used alone or combined with chemotherapy as primary treatment instead of surgery, especially if the size or location of the tumor would make an operation difficult. Doctors may also combine radiation therapy with chemotherapy to shrink the tumor before surgery. Even if the tumor cannot be removed by surgery or destroyed entirely by radiation therapy, radiation therapy can often help relieve pain and make swallowing easier.
- Chemotherapy is the use of anticancer drugs to kill cancer cells. The anticancer drugs used to treat esophageal cancer travel throughout the body. Anticancer drugs used to treat esophageal cancer are usually given by injection into a vein (IV). Chemotherapy may be combined with radiation therapy as primary treatment (instead of surgery) or to shrink the tumor before surgery.
- Laser therapy is the use of high-intensity light to destroy tumor cells. Laser therapy affects the cells only in the treated area. The doctor may use laser therapy to destroy cancerous tissue and relieve a blockage in the esophagus when the cancer cannot be removed by surgery. The relief of a blockage can help to reduce symptoms, especially swallowing problems.
- Photodynamic therapy (PDT), a type of laser therapy, involves the use of drugs that are absorbed by cancer cells; when exposed to a special light, the drugs become active and destroy the cancer cells. The doctor may use PDT to relieve symptoms of esophageal cancer such as difficulty swallowing.
What are the side-effects of treatment?
The side effects of cancer treatment depend on the type of treatment and may be different for each person. Our Doctors and nurses will explain the possible side effects of treatment, and they can suggest ways to help relieve symptoms that may occur during and after treatment.
- Surgery for esophageal cancer may cause short-term pain and tenderness in the area of the operation, but this discomfort or pain can be controlled with medicine. Patients are taught special breathing and coughing exercises to keep their lungs clear.
- Radiation therapy affects normal as well as cancerous cells. Side effects of radiation therapy depend mainly on the dose and the part of the body that is treated. Common side effects of radiation therapy to the esophagus are a dry, sore mouth and throat; difficulty swallowing; swelling of the mouth and gums; dental cavities; fatigue; skin changes at the site of treatment; and loss of appetite.
- Chemotherapy, like radiation therapy, affects normal as well as cancerous cells. Side effects depend largely on the specific drugs and the dose (amount of drug administered). Common side effects of chemotherapy include nausea and vomiting, poor appetite, hair loss, skin rash and itching, mouth and lip sores, diarrhea, and fatigue. These side effects generally go away gradually during the recovery periods between treatments or after treatment is over.
- Laser therapy can cause short-term pain where the treatment was given, but this discomfort can be controlled with medicine.
- Photodynamic therapy makes the skin and eyes highly sensitive to light for 6 weeks or more after treatment. Other temporary side effects of PDT may include coughing, trouble swallowing, abdominal pain, and painful breathing or shortness of breath.